Acne vulgaris remains a pervasive dermatological challenge characterized by overactive innate immune responses, massive leukocyte infiltration, and subsequent tissue damage or scarring. While various treatments exist, there is an increasing demand for safe, effective, and plant-derived candidates to manage acne-prone skin. Panax notoginseng and its bioactive compound Ginsenoside Rh2 (GRh2) were considered as potential solutions due to their ability to modulate key inflammatory signaling pathways, specifically targeting the nodes that drive local inflammation in acne lesions.
Methods
The study utilized chromatographic analysis to identify the chemical profile of P. notoginseng extract and Weighted Gene Correlation Network Analysis (WGCNA) to isolate gene modules significantly correlated with the acne phenotype. Mendelian Randomization (MR) was then performed to establish causal associations between genetically predicted circulating levels of candidate genes and acne risk. Finally, the team conducted in vitro validation using LPS-stimulated RAW264.7 cells to observe the dose-dependent effects of GRh2 on NF-κB activation and cytokine expression.
Key Findings
- Gene Identification: The researchers identified 19 overlapping genes through the integration of differentially expressed genes (DEGs) and WGCNA modules related to acne.
- Pathway Enrichment: Acne pathogenesis was found to be primarily associated with the TNF and IL-17 signaling pathways, which drive cellular responses to bacterial molecules and biotic stimuli.
- The SELE-RELA Axis: Transcription factor p65 (RELA) was identified as the upstream regulator of SELE (E-selectin), a protein that mediates leukocyte adhesion and amplifies inflammatory signaling in skin tissue.
- Protective Decoy: MR analysis suggested that while tissue-bound SELE promotes inflammation, circulating soluble SELE may actually act as a protective decoy to maintain vascular homeostasis.
- Therapeutic Efficacy: Ginsenoside Rh2 (GRh2) was shown to dose-dependently suppress LPS-induced NF-κB/p65 activation and significantly reduce the expression of pro-inflammatory TNF-α.
The novelty of this research lies in its multi-omic approach, combining network pharmacology with Mendelian Randomization to pinpoint the specific GRh2-RELA-SELE regulatory axis in acne treatment. This provides a robust genetic and molecular foundation for using Panax notoginseng derivatives in clinical settings. Future implications include the development of advanced transdermal delivery strategies, such as microneedle-assisted administration, to enhance the bioavailability and localized efficacy of GRh2 for both therapeutic and cosmetic applications.
Link to the study: https://www.sciencedirect.com/science/article/pii/S0926669026011155
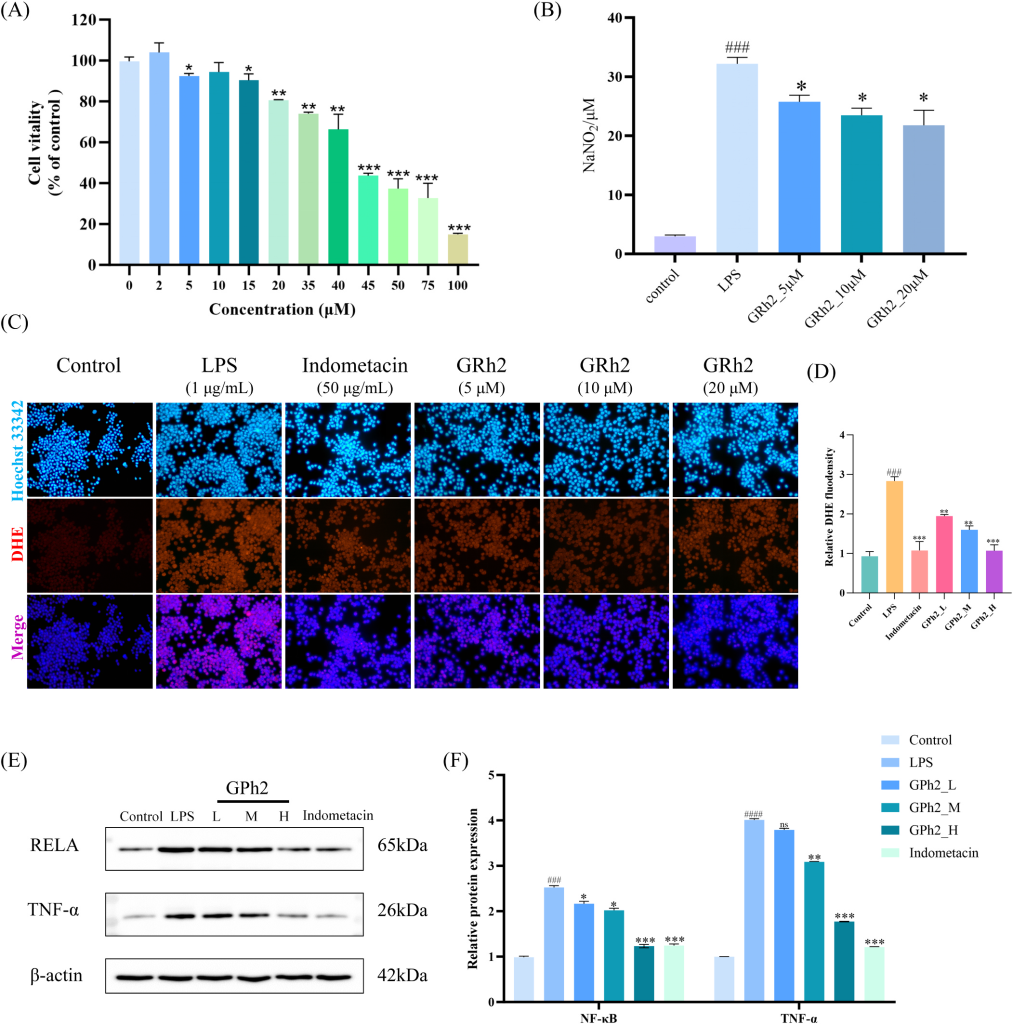
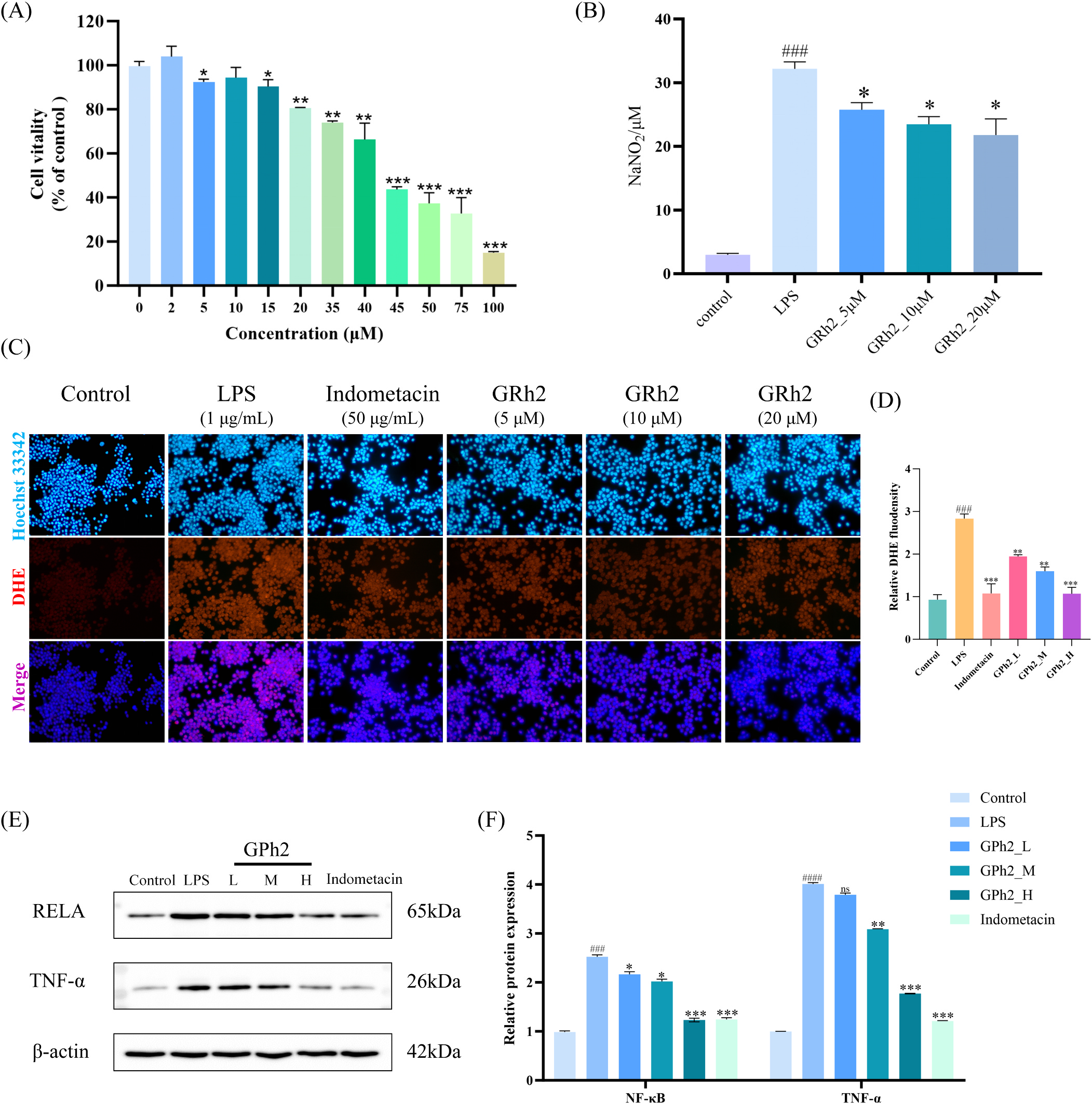
In the figure: Anti-inflammatory effects and underlying mechanisms of Ginsenoside Rh2 in LPS-stimulated RAW264.7 macrophages. (A) Cell viability was assessed
using the CCK 8 assay after treatment with various concentrations of GRh2 (0–100 μM) for 24 h. Data are expressed as a percentage of the untreated control group.
(B) NO production was measured by detecting nitrite accumulation in the culture supernatant using the Griess reaction. Cells were pretreated with GRh2 (5, 10, or
20 μM) for 2 h followed by stimulation with LPS (1 μg/mL) for 24 h. (C) Intracellular ROS levels were visualized by fluorescence microscopy. Cells were stained with
Hoechst 33342 (blue, nuclei) and a ROS-sensitive fluorescent probe (red). Representative images show the Control, LPS model, positive control (Indomethacin,
50 μg/mL), and GRh2 treatment groups (5, 10, and 20 μM). (D) Quantification of ROS levels in cells after treatment. (E, F) Protein expression levels of RELA (NF-κB
p65) and TNF-α were determined by Western blotting. (E) Representative immunoblot bands for RELA, TNF-α, and the loading control β-actin. (F) Quantitative
analysis of relative protein expression normalized to β-actin. L: Low dose (5 μM); M: Medium dose (10 μM); H: High dose (20 μM); + : Positive control (Indomethacin).
Data are presented as mean ± SD (n = 3 independent experiments). Statistical significance was determined by one-way ANOVA followed by post-hoc
tests. *p < 0.05, **p < 0.01, ***p < 0.001 vs. the LPS-only group; # p < 0.05, ### p < 0.001, ####p < 0.0001 vs. the Control group; ns, not significant.